Making Sense of Your Options
A diagnosis of ductal carcinoma in situ (DCIS) can feel overwhelming, but it’s important to remember that this is an early, highly treatable form of breast cancer. The right surgical approach depends on several things: the extent and location of the DCIS, your breast size and shape, and your personal priorities. Your surgical and nursing team will discuss the available choices and help you decide which option best aligns with both your treatment goals and your sense of wellbeing.
Breast-Conserving Surgery (Lumpectomy / Wide Local Excision)
Many women are suitable for breast-conserving surgery, also known as lumpectomy or wide local excision (WLE). This operation removes the area of DCIS together with a small rim of surrounding healthy tissue while preserving the rest of the breast.
Before the operation, the area of DCIS is accurately localized using a fine hookwire or a small magnetic seed. Because DCIS usually cannot be felt by touch, this localization step serves as a “GPS,” guiding the surgeon to accurately identify and remove the affected area during surgery. However, if your DCIS forms a palpable lump (mass-forming DCIS), this step may not be necessary.
This localization is usually done under local anaesthesia, with just a small injection to numb the area.
- Hookwire localization: A thin wire is gently inserted through the skin into the area of concern, usually on the same day as your surgery. A short portion of the wire remains outside the skin and is secured with a small plaster dressing. During surgery, the hookwire is removed together with the affected tissue. (Figure 1b)
- Magnetic seed localization: Instead of a wire, a tiny magnetic seed (about the size of a grain of rice) is placed into the breast at the site of DCIS. The seed can be inserted a few days before surgery, offering greater flexibility and comfort. During the operation, your surgeon uses a special magnetic probe to locate the seed with high precision. However, the use of magnetic seeds depends on availability and is generally more costly than the standard hookwire approach. (Figure 1a)
Both methods are safe and effective, helping ensure that the correct area is removed while preserving as much healthy breast tissue as possible.
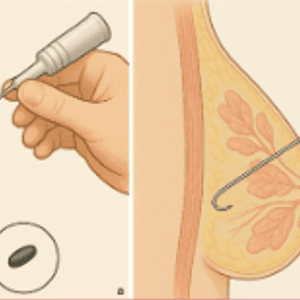
Figure: Illustration showing localization of ductal carcinoma in situ (DCIS) using (a) a magnetic seed or a (b) a hookwire before surgery.
If all the edges (margins) are clear, no further surgery is needed. If any DCIS cells are close to the edge, your surgeon may advise a second operation to ensure complete clearance.
Because a small risk of recurrence remains, radiotherapy is often recommended afterwards. This lowers the chance of DCIS or invasive cancer returning in the same breast.
If a large section of tissue has to be removed, oncoplastic reshaping techniques can help restore a natural breast contour and maintain symmetry. It’s a bit like reshaping the breast from the inside, helping to maintain a smooth contour and good symmetry between both sides, rather than leaving a dent or uneven shape.
Mastectomy and Reconstruction
Sometimes a mastectomy “removal of the whole breast” is the safer choice.
This may be advised when:
- The DCIS affects several parts of the breast, or
- It is too extensive for a good cosmetic outcome with a lumpectomy.
During a mastectomy, your surgeon may also perform a sentinel lymph node biopsy (SLNB) to check whether any invasive cancer cells have travelled to nearby lymph nodes. Only one to three nodes are removed, which limits the risk of arm swelling or stiffness.
If you prefer, breast reconstruction can be done at the same time (immediate) or later (delayed).
Reconstruction options include:
- A silicone implant
- Your own tissue from areas such as the abdomen or back
- A blend of both
Reconstruction is completely optional—it’s about what feels right for you.
Preparing for Surgery
Before your operation, you’ll attend a pre-assessment clinic to make sure you’re fit for general anaesthesia. This means you’ll be completely asleep and pain-free during surgery, while your breathing and vital signs are closely monitored. As part of this assessment, you may have blood tests to check your kidney, liver, and blood cell function, as well as an electrocardiogram and possibly a chest X-ray, to ensure it is safe for you to receive anaesthesia and proceed with the operation.
Your breast care nurse can show you photos of different surgical outcomes and connect you with support groups or other women who have undergone similar procedures.
On the day of surgery, you’ll meet your anaesthetist, who will manage your anaesthesia and pain control. You may also be fitted with compression stockings (TED stockings) to reduce the risk of blood clots.
Recovery After Surgery
Recovery time varies with the type of surgery performed:
- After lumpectomy, most people return home the same day or the following morning.
- After mastectomy, especially with reconstruction, you may stay several days longer.
Your team will encourage you to start gentle arm and shoulder movements soon after the operation to help improve blood circulation, reduce stiffness, and prevent swelling. In some centres, a physiotherapist may guide you through specific exercises to support your recovery and restore comfortable movement.
You’ll have a dressing over your wound, and sometimes a small drain to collect fluid depending on the type of surgery you have undergone. Drains are usually removed within a few days, either before you go home or by a breast care nurse afterwards. Mild bruising, swelling, or a faint bluish tint to the skin (if blue dye was used in node biopsy) or even bluish/greenish tinted urine are commonly expected and will fade with time. Pain is generally well controlled with medication. If discomfort persists, your care team can adjust your pain relief plan.
Before you are discharged, you will be given a hotline number that you can call if you have any concerns or need to contact your healthcare team after going home.
Healing at Home
Your wound may be closed with dissolving stitches or surgical glue, which don’t require removal.
If non-dissolving stitches were used, they’re typically taken out after about a week.
Tiredness is common in the first few weeks.. so listen to your body and rest as needed. Gentle activity such as walking promotes healing. Most women resume daily routines within two to four weeks after lumpectomy and a little longer after mastectomy or reconstruction.
Your nurse will explain how to care for your incision and what to look for.Contact your healthcare team if you notice redness, swelling, warmth, discharge, or fever—these may signal infection and should be checked promptly.
Arm and Shoulder Care
If you’ve had a mastectomy or lymph node removal, you may experience stiffness or heaviness in your shoulder or upper arm. A physiotherapist or nurse will teach you simple arm mobility exercises to prevent tightness and promote flexibility. Occasionally, mild numbness or tingling can occur due to temporary nerve irritation. This usually improves gradually, though a small patch of numbness may persist.
Looking Ahead
Every woman’s recovery unfolds at her own pace. Some feel ready to return to normal activities within weeks; others prefer more time to heal physically and emotionally.
Your follow-up care may include radiotherapy, hormone therapy, or regular mammograms, depending on your specific diagnosis.
Conclusion
At Revivelle Care, your wellbeing remains at the heart of every decision. Our team works closely with you to create a plan that aligns with your medical needs, comfort, and confidence. Recovery doesn’t end in the operating room. It continues through attentive follow-up, rehabilitation, and emotional support, helping you regain strength and balance as you move forward.
Every woman’s experience is unique, but you don't have to figure this out alone. With expert care and compassion, we aim to help you heal not just physically, but wholly. Restoring comfort, confidence, and peace of mind after surgery